After hitting the gym, playing sports, or even going for a run, many athletes turn to protein and amino acid (AA) supplements to enhance muscle recovery and growth. Multiple studies suggest that individuals who regularly exercise or partake in high intensity training require more dietary protein and AAs than sedentary individuals. This additional protein not only allows the human body to repair itself, but is also required for everyday metabolic activities and immune function. Of the twenty amino acids that comprise muscle protein, nine are considered essential amino acids. These essential AAs are not able to be produced by the body on its own, and therefore must be ingested through one’s diet. While it is possible to obtain the necessary protein and nutrients through a regular balanced diet, evidence shows that supplementation before and after exercise may prove advantageous. Among the most popular and cost efficient are powdered proteins, found most commonly in the form of whey and casein. Whey protein, often referred to as “fast” protein, has been shown to elicit a sudden, rapid increase of plasma amino acids following ingestion, providing immediate delivery to the body. Casein, however, is known as “slow” protein and induces a rather progressive and prolonged increase in plasma amino acids. While the digestion of these different proteins has been found to mediate protein metabolism and synthesis after exercise, it is debated whether the use of branched-chain amino acids (BCAAs) augments these processes on its own.
The branched-chain amino acids make up approximately one third of skeletal muscle protein in the body, and account for three of the nine essential AAs. Of the three BCAAs are leucine, isoleucine, and valine, which have laid the foundation for a multi-million dollar industry of nutritional supplements. Distributors of BCAA supplements rave of their anabolic capabilities and claim of their role in muscle recovery when taken post-exercise, particularly in regard to leucine. Leucine has been said to not only act as a precursor for muscle protein synthesis, but also a regulator of intracellular signaling pathways involved in the process of protein synthesis. A few studies have reported that the ingestion of BCAAs increases protein balance either by decreasing the rate of breakdown, increasing the rate of synthesis, or a combination of both. Additionally, it was observed that pairing leucine supplements with carbohydrates and protein before and after workouts led to a heightened level of protein synthesis in the body when compared to trials where leucine was not present. However, the credibility and repeatability of the research behind these claims is unclear, and has been rebutted by other scientific studies.
In this study assessing BCAAs and muscle protein synthesis in humans, the idea that BCAAs alone are capable of promoting muscle anabolism is questioned. This claim has been put forward for more than 35 years, but has been chiefly recorded in rat and other animal studies, with almost no studies being conducted regarding the response to oral consumption. The study involves a detailed literature search, and evaluates the theoretical and empirical data used to make these initial claims regarding BCAAs. It discusses how skeletal muscle in humans comprises a much larger portion of total body mass than in rats and therefore leads to several differences in the way muscle protein synthesis is regulated. Another problem with these previous studies is that they often use the “flooding dose” technique, which involves the administration of an amino acid tracer over a very short time period, therefore neglecting any possibility of sustained effects. With that being said, many of the results found in past experiments employ methods that make the extrapolation of the data to humans unfitting and reduce the physiological significance. In addition, this study displayed how only two studies were conducted analyzing the intravenous effects of BCAAs in humans, noting in both that BCAAs decreased both muscle protein synthesis and protein breakdown. However, the rate of the catabolic processes that broke down muscle protein exceeded the rate of protein synthesis in both cases during BCAA infusion. Due to these findings, the researchers refuted the claim that consumption of dietary BCAAs initiates anabolic activity and increases muscle protein synthesis.
Overall, it is evident that additional attention to diet and supplementation is essential for athletes and individuals who regularly exercise in order to promote the growth and repair of muscles, and to maintain a healthy body. While use of protein powders in the role of muscle protein synthesis has been backed by extensive scientific research, it is still unclear of the extent to which BCAAs are capable of carrying out these same processes on their own. More studies need to be conducted in human subjects observing the activity and metabolism of proteins when dietary BCAAs are ingested to better determine the effectiveness of their use. Many factors come into play when assessing the best supplements to take in regards to exercise, including intake quantity, timing of ingestion, and interaction effects. After observing the conflicting research claims, the use of BCAAs alone may not yield noticeable results, but seems to have little to no risk involved in taking them. Many trainers and workout regimens advise the combination of protein supplements and BCAAs to maximize benefits, but the scientific research is still lacking.
Questions to Consider
What would happen if an individual took more protein supplements/BCAAs than the body needed?
How could studies be better designed to assess the role of BCAAs in humans?
Altitude training has been shown to give athletes a competitive edge by increasing VO2 max, endurance performance, and lung function. The “live high-train low” method as been adopted as one of the most beneficial training methods. By athletes living high and training low, they get the benefits of altitude acclimatization which increases their performance on sea level. As the human body reaches altitude of around 2,100 m, the saturation of oxyhemoglobin decreases significantly. However, a long-term adaptation of living at high altitude is that your body starts to accomodate for the lack of oxygen. By exposing the body to hypoxic conditions, the body will increase its red blood cell (RBC) production as close to 30-50%. This increase in RBCs, increases the oxygen carrying capacity as sea level which will lead to a higher VO2 max, and an increase in athletic performance. An easy and accessible way to simulate altitude training is through the use of altitude training masks.
Elevation Training Mask
Many products have been put on the market in order to simulate high altitude training while training at sea level. One of these products is the “Elevation Training Mask” (ETM). The ETM covers both the nose and mouth, using different sized opening and fluxed valves in order to increase resistance of respiration in hopes of increasing VO2 max and lung function. The resistance system in the masks allows the user to stimulate altitude ranges from 914m to 5486m. But in order to truly stimulate a hypoxic state, the masks would have to be able to decrease the partial pressure of oxygen, questioning if ETMs can truly simulate high altitude training and help with overall performance.
In this study, they tested to see the effects of wearing the ETM on endurance performance variable to conclude if ETMs can act as altitude simulators. Using two groups (a control and those using masks), twenty five subjects completed two, 30 minute, high-intensity workouts per week for 6 weeks. Before and after the 6 week training period, VO2max, ventilatory threshold (VT), peak power output (PPO), respiratory compensation threshold (RCT) and maximal heart rate (MHR) were measured in all subjects. The results are shown in Table 1.
Table 1: Changes in Performance Variables
There was significant improvement in VO2max and PPO in both the control and mask groups. Only the mask group had significant differences in VT, Power Output (PO) at VT, RCT and PO at RCT but improvements in VT and PO at VT did not reach statistical significance (VT p=0.06, PO at VT p=0.170). This study was a well executed study, including pilot testing and constant monitoring of each subject. A limitation of this study is that the subjects volunteered to participate in the study who claimed they were moderately trained. However, the mask and control groups were similar in age, height, weight and BMI at the start of the study. This decreased the amount of variability in the study. Also, the 6 week training period was titrated based on subjects RPE. RPE is a very subjective way to measure intensity and is not always seen to be the most accurate. This however would not skew results significantly. With all this in mind, it is safe to say that the conclusions made from this article are valid. From this study, we can conclude that wearing an EMT during high-intensity workouts does not appear to act as a simulator of altitude, but more like a respiratory muscle training (RMT) device.
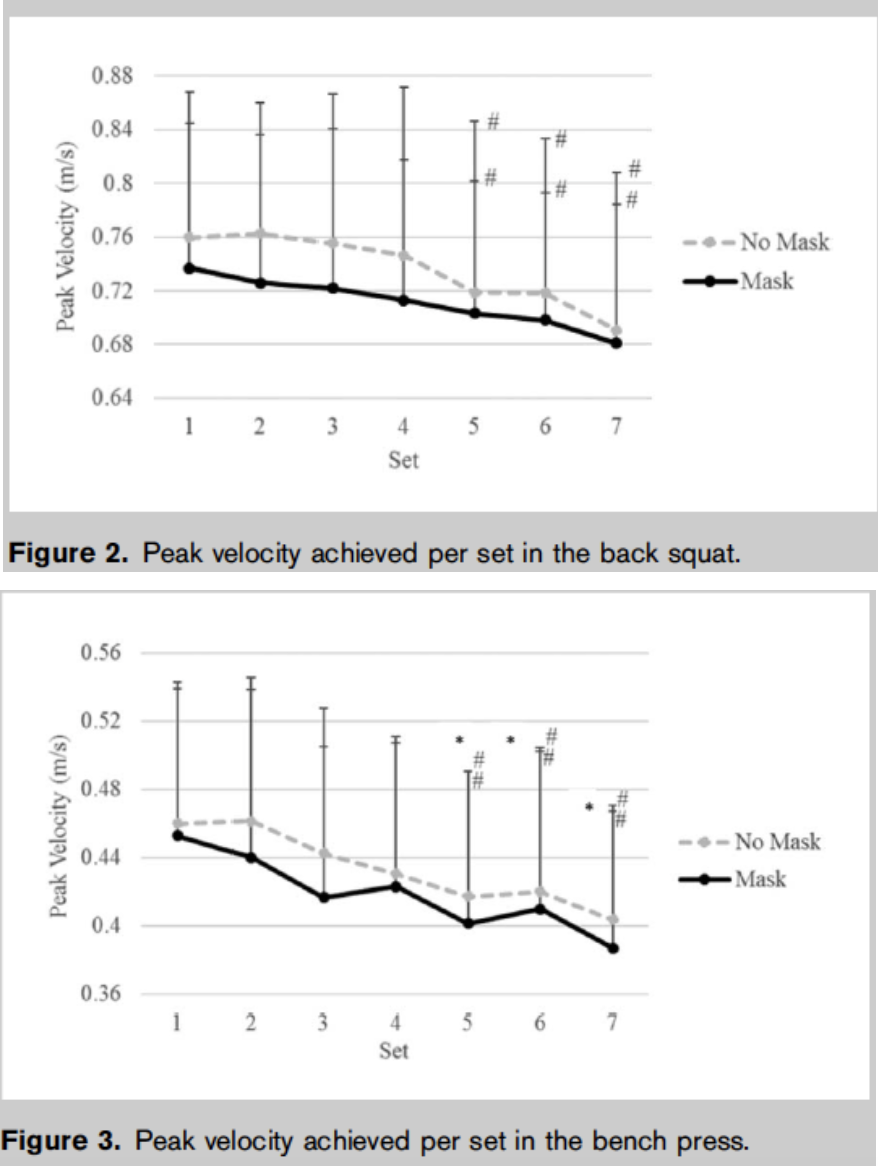
The next study, completed at Lindenwood University is a follow up to the previous study to try and determine if the EMT functions as a RMT device. The study was comprised of 20 recruited resistance-trained men to track the acute effects of the EMT in regards to resistance exercise and maximal effort sprint performances, as well as overall metabolic stress. Baseline testing was completed 3-7 days before the subjects experimental results were obtained. These tests were used to determine the subjects body composition and to assess their 5-repetition maximum (5RM) for bench press and back squat after they were appropriately familiarized with the equipment (bench press, squat rack and non-motorized treadmill). Two trials for all subjects were completed on non-consecutive days with and without the mask (EMT and No Mask (NM) conditions, respectively). The subjects were to complete a bench press and back squat (using weight based off their individual 5RM), as well as a 25-second all out sprint test. Velocity of the bars for the bench and squat tests were determined using a linear position transducer (accuracy correlation coefficient of 0.97). Blood samples were collected to determine blood lactate and oxygen saturation was determined using a finger pulse oximeter. ANOVA was used for statistical analysis to compare the EMT and NM conditions. Peak velocity of the bench press and back squat were significantly greater in the NM trial (both p = 0.04 < 0.05). Blood lactate was higher in the NM condition for the bench press and sprint test (p < 0.001). Using a 5-point Likert scale to the subjects self-selected their energy, fatigue, alertness and focus for both conditions. The EMT surprisingly did not differ significantly from the NM condition. It should also be noted that 3 subjects were unable to complete the protocols using the EMT masks due to extreme discomfort and their results were omitted from the study. Contrary to the original hypothesis, the EMT condition did not significantly decrease the amount of bench and squat repetitions completed to failure. It was confusing, however, that the blood lactate was found to be higher for the NM condition. It would be expected, since the mask’s purpose is to restrict the user’s access to oxygen, that the EMT group’s blood lactate would be higher since less oxygen would lead to more anaerobic respiration and therefore more lactate. The researchers attribute this phenomenon to less fast twitch fibers being recruited, which explains why the velocity for the bench and squat were lower for the EMT condition. They also admit that more studies need to be completed before that claim can be made.
Overall, this study was well controlled. All subjects diets were monitored carefully before all testing, and all results were obtained in a relatively consistent manner. However, using a 5-Point Likert scale opens the study up to subjective bias, especially since the subjects were not blinded to the different test conditions (they were consciously aware of wearing the mask). Also, the long-term aim of this study seems to be a little unclear. They mentioned in the introduction they wanted to see if the masks could serve as a RMT device, but only measured the acute responses. The effects of the EMT on respiratory muscle function would probably not be seen after weeks or even months after training. All in all, the study yielded few significant results to support that EMTs can acutely affect respiration at an anaerobic capacity.
Both studies were able to conclude that the EMTs did not completely mimic an environment of higher elevation. As mentioned previously, this probably has to do with the EMT’s inability to alter the partial pressure of oxygen. The first study had indicated that the mask served more as an RMT device, rather than a simulator of altitude. The second study, however, did not obtain results to support this claim. Elevation masks are a relatively new technology, and more extensive studies will need to take place before any conclusive claims can be made. Studies in the future, should probably follow the first’s with studying the effects long-term, rather than one time use. Additional studies lasting weeks or even months will be able to determine if EMTs have any long lasting effects on aerobic capacity and respiratory muscle function with training.
Questions to Consider
How can Elevation Masks be designed differently to alter the partial pressure of oxygen?
Do EMTs have any negative effects on the brain (oxygen deprivation, ect.)?
What effects to EMTs have on the different portions of the respiration system (i.e. lungs, gas exchange, ect.)?
Cupping is form of alternative medicine that is said to help with pain, inflammation and blood flow. All of this can lead to better well-being and relaxation as it acts as a form of deep tissue massage. While not that popular, you may have seen it being used during the Rio Summer Olympic games in 2016. Many athletes, such as Michael Phelps, were seen with large purple spots along their body. This is the result of cupping therapy. Cupping is usually put into two categories; wet and dry. Dry cupping involves the suction of the skin into the cup. Wet cupping has one extra step in which an incision is made, and blood is drawn from the suctioned area. While Olympic athletes seem convinced, is there any scientific data to support cupping as a valid therapy for recovery and rehabilitation?
First, we will look into rehabilitation. A study from Evidence-Based Complementary and Alternative Medicine attempted to prove the efficacy of cupping therapy for treating chronic neck and shoulder pain. The three things that they were looking for was skin surface temperature, blood pressure, and pain intensity. They had a cupping and a control group and found cupping to be statistically significant in raising the skin surface temperature and lowering the pain intensity (Figure 1). The conclusion was that cupping causes vasodilation and can increase blood circulation and is therefore an effective therapy for chronic neck and shoulder pain. These results are not without some cause for concern. First off the sample size was relatively small and similar. Also the increase in skin surface temperature is to be expected, however the pain intensity could be attributed to a number of things. Pain tolerance between patients is different and the decrease in pain intensity of the cupping group could be a result of the placebo effect.
One case study looked into utilizing cupping therapy as a means of treatment for vascular thoracic outlet syndrome. Vascular thoracic outlet syndrome is when blood vessels and nerves near the collarbone are compressed. This restricts blood flow and can lead to pain and numbness along the shoulder and down to the fingers. The case study focused on a collegiate baseball pitcher who had been diagnosed with the disease. The pitcher was put on a program that included cupping therapy on alternating days combined with certain range of motion exercises. The patient began to pitch again and noted no swelling, increased range of motion and significantly less pain. All of this would suggest that the cupping therapy was effective in treating this ailment. However, some issues with the case study is that they did not continue to follow up with the patient after the 3 week period and the sudden improved health could be attributed to a number of different factors. The authors do admit that more research and testing must be conducted to fully understand the efficacy of cupping therapy.
In regards to recovery, a study was done by a team of Greek researchers to find how cupping therapy compares to other treatments in the combating of myofascial pain syndrome. Myofascial pain syndrome is caused by painful spots in the fascia surrounding the skeletal muscle due to repetitive injury, training overload, and muscular overuse. Cupping was done to 20 amateur soccer athletes once a week for three weeks, and their pain pressure threshold (PPT) and visual analogue scale (VAS) was taken before and after the treatment sessions. An increase in PPT and a decrease in VAS was observed in the athletes after cupping. These changes suggest that cupping does have an effect on the body. It’s stated in the article that researchers believe cupping causes hyperemia and local stretching, which is similar to what the first study concluded.
These results show that cupping seems to improve recovery, however other recovery techniques appear to be more effective. Cupping saw the smallest change in the pre and post values. Additionally, it’s always important to consider each participant’s pain tolerance varies. This helps to explain why the standard deviation was ~1.5 for all values in table one.
Compiling all of the evidence, it seems cupping does have an effect on rehabilitation and recovery. Cupping causes vasodilation and hyperemia. This increase in blood circulation and dilation of the blood vessels helps to combat illness that are caused by constricted/compressed blood vessels, like vascular thoracic outlet syndrome. According to the third article though, cupping may not be the most effective recovery solution. When considering the cost of each treatment method, availability, and preference, cupping may not always be the best solution for recovery.
Questions to Consider:
When would cupping therapy be ideal to use?
How is cupping therapy better than other therapies?
Can cupping therapy be combined with other techniques to boost its performance?
Further Readings/References:
Ahmadi, Alireza, et al. “The Efficacy of Wet-Cupping in the Treatment of Tension and Migraine Headache.” The American Journal of Chinese Medicine, vol. 36, no. 01, 2008, pp. 37–44., doi:10.1142/s0192415x08005564.
Bridgett, Rhianna, et al. “Effects of Cupping Therapy in Amateur and Professional Athletes: Systematic Review of Randomized Controlled Trials.” The Journal of Alternative and Complementary Medicine, vol. 24, no. 3, 2018, pp. 208–219., doi:10.1089/acm.2017.0191.
Jun, Wu. “Experimental Study on Treatment of Chronic Soft Tissue Injuries with Fire-Needle Therapy.” Chinese Acupuncture & Moxibustion, 2002, doi: R245.316.
After talking briefly about muscle stretch shortening in class, I thought this was an interesting topic and looked into some literature to better understand what is going on. I found a study that focused on upper-body explosive movements, and how load and stretch shortening cycles (SSC) affect the kinematics, kinetics, and muscle activation that occur. This was an interesting study because they looked at maximal effort bench throws, where much of the previous research focused only on lower-extremity exercises. Each subject performed an SSC throw and concentric only throws, comparing displacement, velocity, acceleration, force, power output and EMG from the pectoralis major, anterior deltoid, and triceps brachii. SSCs are usually performed before explosive movements (e.g. throwing, jumping) which lengthen the muscle preparing to contract to ensure maximal velocity is reached during the movement. When the muscle lengthens, elastic energy is stored which can then be released during the movement, however, if the time between lengthening and contracting is too long, the energy dissipates, leading to a slower contraction with less power.
As expected, the average velocity was lower for the concentric only throws when compared to the SSC throws, however, there was no difference in throw height between the two groups. Average and peak force and power output were both higher for the SSC through compared to the concentric only throw. The findings from this study agree with findings from previous studies focusing on vertical jump, showing that similar muscle kinetics are at play. Muscle kinetics are an extremely interesting area of study, and even though we only briefly discussed muscle length-tension, force-velocity, and power relationships in class, this is a huge field of study. Some groups choose to look at specific muscle groups, while others look at more complex movements that require multiple groups of muscles to be activated. This area of research has led to improvements in stretching suggestions for athletes; stretching before performing explosive movements is not actually as beneficial as we once thought. Stretching the muscle allows for elastic energy dissipation, instead of storing the energy for immediate release. However, stretching is still extremely beneficial after workouts, helping to prevent muscle soreness and excess inflammation. Additionally, there are some chronic adaptations to stretching including increasing flexibility for a wider range of motion during typical daily activities as well as athletic endeavors.
References:
Newton, R. U., Murphy, A. J., Humphries, B. J., Wilson, G. J., Kraemer, W. J., & Häkkinen, K. (1997). Influence of load and stretch shortening cycle on the kinematics, kinetics and muscle activation that occurs during explosive upper-body movements. European Journal of Applied Physiology and Occupational Physiology, 75(4), 333–342. https://doi.org/10.1007/s004210050169
Bosco, Carmelo, and Paavo V. Komi. (1979) Mechanical characteristics and fiber composition of human leg extensor muscles. European journal of applied physiology and occupational physiology4 (1979): 275-284.
A major choice when deciding what workout to do is whether to use machines or free weights. Machines are typically resistance training devices that have cables, adjustable weight stacks, and levers to customize workouts for the user in a controlled manner, while free weight exercises are more ‘free-form’ and involve using dumbbells or plates on utility benches or squat racks. Some people may prefer machines because the workouts are guided, as the machine controls the path of motion of the weight and has diagrams to properly explain how to use the machine. However, free weights are more similar to real-life movement patterns, requiring the same types of forces common in daily activities and sports. So how should you choose which workout style is best? This depends on what your goal is. So first, we’ll talk about the pros and cons of both machines and free weights.
There are several studies that have looked at the pros and cons of free weights and machines, with this round table discussion being the most interesting. Free weights are inherently unguided, so when performing exercises, like squatting with a barbell, not only are the muscles to lift the weight required, but also the supporting muscles to help you balance and stabilize while you perform the squat are active. Using free weights directly translates to typical daily activities, like lifting bags of groceries or unloading heavy items from a car, as mentioned by McBride. Additionally, free weights are typically less expensive to purchase and maintain than machines because they only require the actual weight, not a large piece of equipment to guide and apply the weight. Once purchased, free weights can be more cost effective than machines because they don’t have any moving parts that need to be greased or cleaned, or cables that may break if rust accumulates. Another advantage to free weights is that they come in many different shapes and sizes, so they are more customizable for the individual as there is no minimum or maximum height requirement to use free weights, and the same weights can be used for multiple different types of exercises.
Free weights come in different shapes and sizes so workouts can be adjusted for the individual.
Free weights sometimes require using a spotter and special racks to hold the weights.
However, free weights can often be intimidating for novice users because they require knowledge of different types of exercises, as well as understanding how heavy the weights should be for these different exercises to prevent injury while still seeing results. Some free weight exercises, like bench presses, are best performed with spotters and special racks, so this may add additional cost as well as requiring another person to work out with you, which is not always convenient. Another disadvantage to free weights is that they often require more space than machines; ample room is required surrounding the individual using free weights to avoid hitting anyone or anything while performing exercises.
On the other hand, machines are attractive to novice weight lifters and athletes and are very user-friendly. As mentioned previously, machines are advantageous because they control the movement of the exercise. This controlled movement guides users to perfect form and minimizes potential for injury. Additionally, machines bear utility for injured persons who still seek to exercise uninjured areas but cannot move free weights into the necessary start position due to their injuries. Still further, machines allow users to quickly change weights between sets, making for a more efficient workout. Lastly, machine users never require a spotter and thus allow athletes to exercise safely alone, a major pro mentioned in the round table discussion.
Machines guide the user’s motion during exercise, decreasing risk of injury.
Cables and pulleys on machines can wear over time, increasing the cost of maintenance for exercise equipment.
One drawback of machines is their high cost, as they are significantly more expensive than free weights on average. Due to the guided load path offered by machines, they suffer from limited stabilizer muscle activation. Additionally, machines typically isolate single muscle groups, which does not allow for explosive training. Further, the isolated nature of machines does not mimic real world movements or lift patterns.
In conclusion, if you desire an effective workout and prefer to workout alone and have no cost limit, machines may be the best choice for you. However, if you like to workout with a partner or are short on funds, free weights may be the better choice. Both workout types show results when utilized correctly, so be sure to experiment with both machines and free weights to find the workout type that works for you!
Questions to Consider:
Are there any sports that would soley benefit from one lifting modality versus the other?
If you’re trying to isolate muscle groups in the legs, would you benefit more from a machine or free weight workout?
In your experience, do you find machines or free weights more user friendly? Do you find either to give you a more satisfying workout?
References for Further Reading:
Haff, G. G. (2000). Roundtable Discussion: Machines Versus Free Weights. Strength and Conditioning Journal, 22(6), 18. https://doi.org/10.1519/1533-4295(2000)022<0018:RDMVFW>2.0.CO;2
McBride JM. Machines versus free weights. NSCA Hot Topic Series. Available from: http://www.nsca-lift.org.
McCaw, Steven T., and Jeffrey J. Friday. “A comparison of muscle activity between a free weight and machine bench press.” J Strength Cond Res 8.4 (1994): 259-64.
Santana, Juan Carlos. “Machines versus Free Weights.” Strength & Conditioning Journal 23.5 (2001): 67.

 nched-chain amino acids (BCAAs) augments these processes on its own.
nched-chain amino acids (BCAAs) augments these processes on its own. revious studies is that they often use the “flooding dose” technique, which involves the administration of an amino acid tracer over a very short time period, therefore neglecting any possibility of sustained effects. With that being said, many of the results found in past experiments employ methods that make the extrapolation of the data to humans unfitting and reduce the physiological significance. In addition, this study displayed how only two studies were conducted analyzing the intravenous effects of BCAAs in humans, noting in both that BCAAs decreased both muscle protein synthesis and protein breakdown. However, the rate of the catabolic processes that broke down muscle protein exceeded the rate of protein synthesis in both cases during BCAA infusion. Due to these findings, the researchers refuted the claim that consumption of dietary BCAAs initiates anabolic activity and increases muscle protein synthesis.
revious studies is that they often use the “flooding dose” technique, which involves the administration of an amino acid tracer over a very short time period, therefore neglecting any possibility of sustained effects. With that being said, many of the results found in past experiments employ methods that make the extrapolation of the data to humans unfitting and reduce the physiological significance. In addition, this study displayed how only two studies were conducted analyzing the intravenous effects of BCAAs in humans, noting in both that BCAAs decreased both muscle protein synthesis and protein breakdown. However, the rate of the catabolic processes that broke down muscle protein exceeded the rate of protein synthesis in both cases during BCAA infusion. Due to these findings, the researchers refuted the claim that consumption of dietary BCAAs initiates anabolic activity and increases muscle protein synthesis. 








{kind=link}