
Eric Bartholomew and Joe Yovanovich
Altitude training has been shown to give athletes a competitive edge by increasing VO2 max, endurance performance, and lung function. The “live high-train low” method as been adopted as one of the most beneficial training methods. By athletes living high and training low, they get the benefits of altitude acclimatization which increases their performance on sea level. As the human body reaches altitude of around 2,100 m, the saturation of oxyhemoglobin decreases significantly. However, a long-term adaptation of living at high altitude is that your body starts to accomodate for the lack of oxygen. By exposing the body to hypoxic conditions, the body will increase its red blood cell (RBC) production as close to 30-50%. This increase in RBCs, increases the oxygen carrying capacity as sea level which will lead to a higher VO2 max, and an increase in athletic performance. An easy and accessible way to simulate altitude training is through the use of altitude training masks.

Elevation Training Mask
Many products have been put on the market in order to simulate high altitude training while training at sea level. One of these products is the “Elevation Training Mask” (ETM). The ETM covers both the nose and mouth, using different sized opening and fluxed valves in order to increase resistance of respiration in hopes of increasing VO2 max and lung function. The resistance system in the masks allows the user to stimulate altitude ranges from 914m to 5486m. But in order to truly stimulate a hypoxic state, the masks would have to be able to decrease the partial pressure of oxygen, questioning if ETMs can truly simulate high altitude training and help with overall performance.
In this study, they tested to see the effects of wearing the ETM on endurance performance variable to conclude if ETMs can act as altitude simulators. Using two groups (a control and those using masks), twenty five subjects completed two, 30 minute, high-intensity workouts per week for 6 weeks. Before and after the 6 week training period, VO2max, ventilatory threshold (VT), peak power output (PPO), respiratory compensation threshold (RCT) and maximal heart rate (MHR) were measured in all subjects. The results are shown in Table 1.

Table 1: Changes in Performance Variables
There was significant improvement in VO2max and PPO in both the control and mask groups. Only the mask group had significant differences in VT, Power Output (PO) at VT, RCT and PO at RCT but improvements in VT and PO at VT did not reach statistical significance (VT p=0.06, PO at VT p=0.170). This study was a well executed study, including pilot testing and constant monitoring of each subject. A limitation of this study is that the subjects volunteered to participate in the study who claimed they were moderately trained. However, the mask and control groups were similar in age, height, weight and BMI at the start of the study. This decreased the amount of variability in the study. Also, the 6 week training period was titrated based on subjects RPE. RPE is a very subjective way to measure intensity and is not always seen to be the most accurate. This however would not skew results significantly. With all this in mind, it is safe to say that the conclusions made from this article are valid. From this study, we can conclude that wearing an EMT during high-intensity workouts does not appear to act as a simulator of altitude, but more like a respiratory muscle training (RMT) device.
The next study, completed at Lindenwood University is a follow up to the previous study to try and determine if the EMT functions as a RMT device. The study was comprised of 20 recruited resistance-trained men to track the acute effects of the EMT in regards to resistance exercise and maximal effort sprint performances, as well as overall metabolic stress. Baseline testing was completed 3-7 days before the subjects experimental results were obtained. These tests were used to determine the subjects body composition and to assess their 5-repetition maximum (5RM) for bench press and back squat after they were appropriately familiarized with the equipment (bench press, squat rack and non-motorized treadmill). Two trials for all subjects were completed on non-consecutive days with and without the mask (EMT and No Mask (NM) conditions, respectively). The subjects were to complete a bench press and back squat (using weight based off their individual 5RM), as well as a 25-second all out sprint test. Velocity of the bars for the bench and squat tests were determined using a linear position transducer (accuracy correlation coefficient of 0.97). Blood samples were collected to determine blood lactate and oxygen saturation was determined using a finger pulse oximeter. ANOVA was used for statistical analysis to compare the EMT and NM conditions. 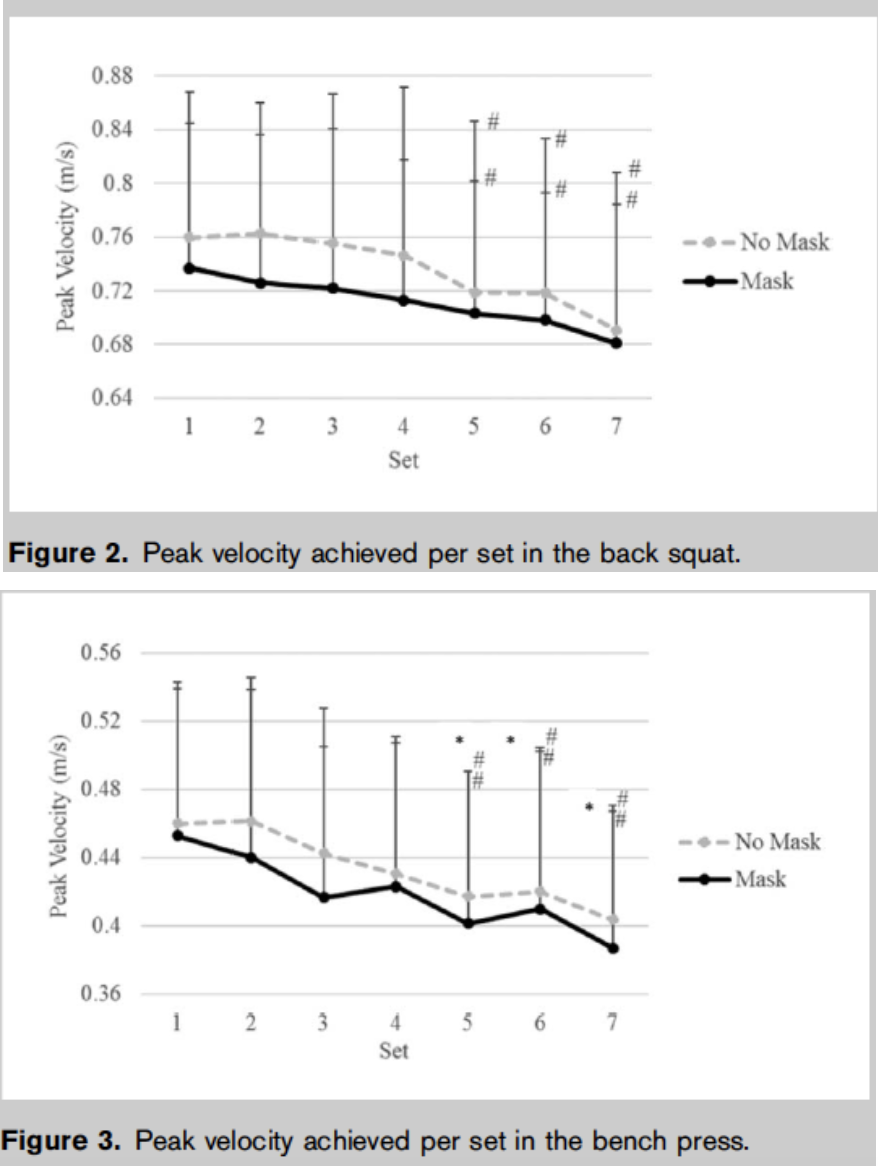 Peak velocity of the bench press and back squat were significantly greater in the NM trial (both p = 0.04 < 0.05). Blood lactate was higher in the NM condition for the bench press and sprint test (p < 0.001). Using a 5-point Likert scale to the subjects self-selected their energy, fatigue, alertness and focus for both conditions. The EMT surprisingly did not differ significantly from the NM condition. It should also be noted that 3 subjects were unable to complete the protocols using the EMT masks due to extreme discomfort and their results were omitted from the study. Contrary to the original hypothesis, the EMT condition did not significantly decrease the amount of bench and squat repetitions completed to failure. It was confusing, however, that the blood lactate was found to be higher for the NM condition. It would be expected, since the mask’s purpose is to restrict the user’s access to oxygen, that the EMT group’s blood lactate would be higher since less oxygen would lead to more anaerobic respiration and therefore more lactate. The researchers attribute this phenomenon to less fast twitch fibers being recruited, which explains why the velocity for the bench and squat were lower for the EMT condition. They also admit that more studies need to be completed before that claim can be made.
Peak velocity of the bench press and back squat were significantly greater in the NM trial (both p = 0.04 < 0.05). Blood lactate was higher in the NM condition for the bench press and sprint test (p < 0.001). Using a 5-point Likert scale to the subjects self-selected their energy, fatigue, alertness and focus for both conditions. The EMT surprisingly did not differ significantly from the NM condition. It should also be noted that 3 subjects were unable to complete the protocols using the EMT masks due to extreme discomfort and their results were omitted from the study. Contrary to the original hypothesis, the EMT condition did not significantly decrease the amount of bench and squat repetitions completed to failure. It was confusing, however, that the blood lactate was found to be higher for the NM condition. It would be expected, since the mask’s purpose is to restrict the user’s access to oxygen, that the EMT group’s blood lactate would be higher since less oxygen would lead to more anaerobic respiration and therefore more lactate. The researchers attribute this phenomenon to less fast twitch fibers being recruited, which explains why the velocity for the bench and squat were lower for the EMT condition. They also admit that more studies need to be completed before that claim can be made.
Overall, this study was well controlled. All subjects diets were monitored carefully before all testing, and all results were obtained in a relatively consistent manner. However, using a 5-Point Likert scale opens the study up to subjective bias, especially since the subjects were not blinded to the different test conditions (they were consciously aware of wearing the mask). Also, the long-term aim of this study seems to be a little unclear. They mentioned in the introduction they wanted to see if the masks could serve as a RMT device, but only measured the acute responses. The effects of the EMT on respiratory muscle function would probably not be seen after weeks or even months after training. All in all, the study yielded few significant results to support that EMTs can acutely affect respiration at an anaerobic capacity.
Both studies were able to conclude that the EMTs did not completely mimic an environment of higher elevation. As mentioned previously, this probably has to do with the EMT’s inability to alter the partial pressure of oxygen. The first study had indicated that the mask served more as an RMT device, rather than a simulator of altitude. The second study, however, did not obtain results to support this claim. Elevation masks are a relatively new technology, and more extensive studies will need to take place before any conclusive claims can be made. Studies in the future, should probably follow the first’s with studying the effects long-term, rather than one time use. Additional studies lasting weeks or even months will be able to determine if EMTs have any long lasting effects on aerobic capacity and respiratory muscle function with training.
Questions to Consider
- How can Elevation Masks be designed differently to alter the partial pressure of oxygen?
- Do EMTs have any negative effects on the brain (oxygen deprivation, ect.)?
- What effects to EMTs have on the different portions of the respiration system (i.e. lungs, gas exchange, ect.)?
References/Further Reading
[1] Porcari, John P., et al. “Effect of Wearing the Elevation Training Mask on Aerobic Capacity, Lung Function, and Hematological Variables” Journal of Sports Medicine and Science, Online, 15(2): 379-386, 2016.
[2] Jagim, AR, Dominy, TA, Camic, CL, Wright, G, Doberstein, S, Jones, MT, and Oliver, JM. “Acute effects of the elevation training mask on strength performance in recreational weightlifters”. Journal of Strength and Conditioning Research, Online, 32(2): 482-489, 2018.
{kind=link}
[5] Effects of Simulated Altitude on Maximal Oxygen Uptake and Inspiratory Fitness

I have seen a few people sporting these masks in the gym, and always wondered whether they were really doing anything beneficial. From what I’ve heard and from what you guys said above, it seems that these masks simply make breathing harder by reducing the amount of airflow into the lungs, but have no pronounced effect on endurance or performance. I would be surprised if there was a practical technology on the market capable of simulating high altitudes and producing the same physiological adaptations on the body. As many studies have shown, it takes weeks to months of living and training at high altitudes to observe these adaptations, so it would be foolish to believe that wearing a mask for an hour long training session a few times a week would prove advantageous. Particularly for athletes focusing on short duration, high intensity activities like weightlifting, these masks may even be detrimental, since oxygen utilization is much less of a determinant of performance and requires more anaerobic processes.
I agree, it seems like this technology is not that practical. To gain the most benefits, I think you’d have to wear the mask not only when you’re exercising, but also during normal activities, which would be hard to do. Additionally, I think the mask would be most effective during cardio exercises like running, but with the high impact forces during running and the jostling that occurs, I imagine the mask would slip out of place, or would be very uncomfortable like the masks worn during VO2max tests.
I definitely agree that training with this mask most likely will not have any positive long term effects. Going off the ‘live high train low’ mantra, I wonder what the effects of wearing the mask during rest activities and even while sleeping and then training without the mask would be?
In the blog post you mentioned that the EMT would be considered an RMT device as opposed to simulating altitude triaining? Is altitude training not considered a form of an RMT? If not what are the different characteristics that would define one thing as a RMT?
They would run a study where all participants wear “mask” but only one is functional to remove the participant bias. To get accurate data, they would probably have to wear them for weeks or whenever adaptations would begin. Michael Phelps slept in an altitude chamber to improve his performance, but it is easier to change the partial pressure of oxygen in a room than a small mask. As technology progresses, the masks will probably be more efficient. Since the adaptations happen over time, there most likely wouldn’t be a huge difference without proper training. Are there any thoughts on if pressure chambers or masks would be an unfair advantage?
As others have mentioned, further studies should be conducted to determine the long term effects of wearing these masks. It would be interesting if these studies looked at the brain in addition to the respiratory system to determine any chronic adaptations. If the point of the masks is to mimic high altitude, there shouldn’t be any negative effects from oxygen deprivation, but as you’ve pointed out, the masks work more as RMT devices.
Even though the masks are not able to capture the conditions of training at altitude would it still be beneficial for endurance athletes to use them if they are considered a respiratory training device?
Very interesting topic. I have seen these elevation masks used, and I always thought they just looked silly, especially when I have seen most people doing heavy weight training, opposed to more cardiovascular respiratory training. I wonder if this could potentially benefit football teams when they are going to play at a higher elevation? For example, when teams visit the Denver Broncos they often are seen gassed, using oxygen breathing masks on the sidelines. I think this technology might be able to help.
I think it’s interesting to consider the possibility of these masks being detrimental (via oxygen deprivation as you have mentioned in your question). I think it is quite possible, as the research did conclude that the masks do not totally mimic the environment desired. However, I think the degree of damage that these could cause would have to be more closely examined and would be a great topic for a future research study.
Interesting point Cassie. Conclusions from the study appear to show that although the masks restrict airflow, they do not successfully decrease the partial pressure of oxygen: as seen in high elevation environments. I’d be interested to look further as to what happens on an alveolar level. The decreased partial pressure may significantly decrease the effectiveness of gas exchange, therefore the body needs to produce RBCs to keep up. My question would be do these masks really effect the efficiency of gas exchange? If not, do the users only just breath at a more rapid rate to try to make up for the loss of volume with each breath? If so, I can definitely see the possibility of users suffering from hyperventilation, which can have detrimental health effects.