
Most athletes have heard the term, “no pain, no gain” at one point or another in their athletic careers, but this saying is truer than one might think. Having grown up in a household where sports were played year round, it was common to take over the counter non-steroidal anti-inflammatory drugs (OTC NSAIDs), such as ibuprofen or aspirin to ease the pain. Ran too far? Easy solution, take some Advil. Overdo it with the lifting? Take a few Motrin and you’ll be ready in the morning. It was even common to take these over the counter drugs before a workout, as a way to get a head start on the pain.

Ibuprofen, a common OTC NSAID.
Is there any validity to this solution? OTC NSAID’s are known for their ability to reduce fevers and minor aches and pains. With that being said, are they really useful for exercise related injuries or pains? Specifically, are they safe and effective to use for delayed onset muscle soreness (DOMS) due to exercise?
DOMS is the pain and stiffness that is felt typically between 24 and 72 hours after the workout has been completed but can last up to 7 days. After a strenuous workout, the body responds with acute inflammation as a natural way to heal the body. This inflammation usually goes hand in hand with DOMS, but the specifics of this relationship have not been clearly defined. Many athletes try to combat this by taking ibuprofen (or other OTC NSAIDs) to ease the pain, but recent studies have shown that this isn’t necessarily a foolproof plan.
In a 2006 study completed by Nieman et al., the influence of ibuprofen was measured during the 160-km Western States Endurance Run on endotoxemia (the presence of endotoxins in the blood), inflammation and plasma cytokines. The study included 29 ultramarathoners who consumed 600 and 1200mg ibuprofen the day before and on the race day, respectively, and 25 controls that competed in the race but did not take ibuprofen or any other medications. Blood and urine samples were collected the morning prior to and immediately following the race, and subjects recorded muscle soreness during the week following the race using a 10-point Likert scale. It was found that ibuprofen use compared to non-users did not alter muscle soreness or damage. In addition ibuprofen use was linked to elevated indicators of endotoxemia and inflammation. One limitation of the study was that it did not have a placebo group due to ethical concerns from the race director, but they may have had an impact on the results. In addition, race conditions are not the best conditions to conduct an experiment under, as they can cause extra stress on the body, affecting the results.
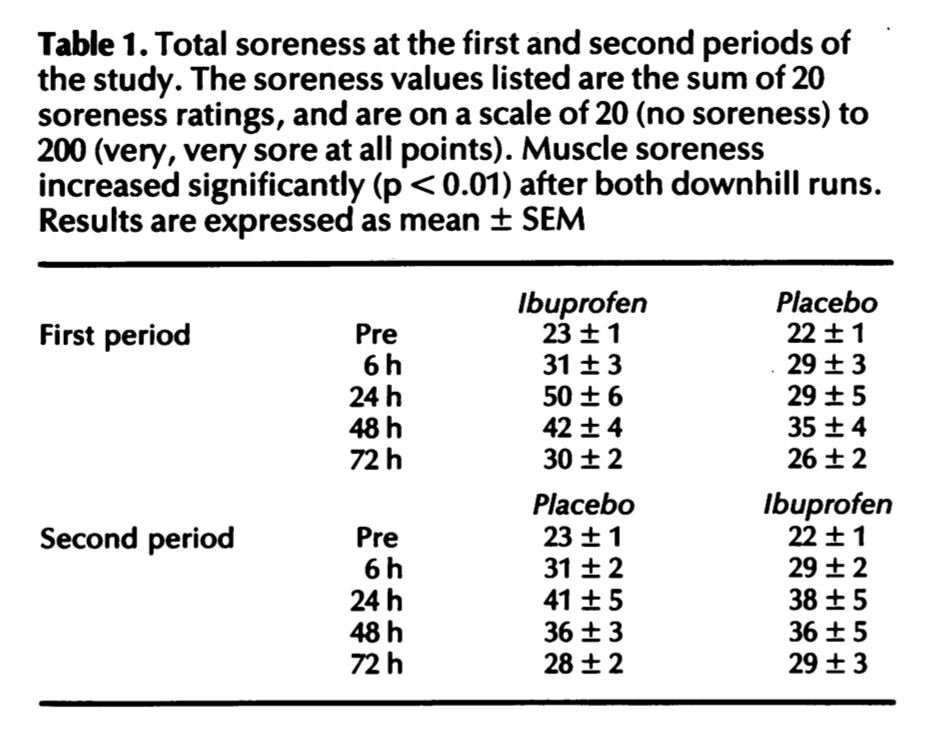
In another study conducted by Donnelly et al., 32 volunteers participated in a study in which ibuprofen was tested against an identical placebo for its effectiveness in reducing muscle soreness and damage after two periods of downhill running. Volunteers took two 600mg ibuprofen or placebo tablets 30 minutes before each run, and took one 600mg tablet every six hours up to 72 hours post-exercise. Blood samples were drawn pre- and post-exercise, and at 6, 24, 48 and 72 hours and analyzed for indicators of muscle damage and inflammation. A questionnaire was used to determine muscle soreness for different regions of the body (the results can be seen in Table 1). The results indicated that ibuprofen is not an appropriate treatment for DOMS and muscle damage. However, one limitation of this study was that during the 10 week break between the two periods of running, there was no monitoring or control of the participants, which means their lifestyles could have been very different from each other, thereby affecting the results.
Furthermore, it is known that exhaustive physical activity leads to small intestinal injury and short-term loss of gut barrier function in otherwise healthy individuals. Another study, conducted in 2012 reveals that ibuprofen aggravates this exercise-induced small intestinal injury and induces gut barrier dysfunction in healthy individuals.
Based on this research, I have concluded that OTC NSAIDs should be discouraged as a way to mitigate the pain that comes with delayed onset muscle soreness. The data from the first two studies show that ibuprofen (and implied other NSAIDs) are not a satisfactory way to decrease the pain that comes from delayed onset muscle soreness. The third study shows that ibuprofen can be extremely harmful to the user and therefore should not be taken if it can be avoided. Based on this information, not only should OTC NSAIDs not be taken for DOMS, but the relationship between inflammation and DOMS should be more thoroughly investigated. It could be that the inflammation isn’t causing DOMS and that is why the drugs aren’t relieving the pain. However, the first study suggests that the intake of ibuprofen increased inflammation, the exact opposite of what it was supposed to do. Either way, ibuprofen and other NSAIDs should not be taken for relief from DOMS.
Questions to consider:
Do you take OTC NSAIDs such as ibuprofen or Advil when you are feeling sore after a hard workout? Do they help? Will you continue?
How often do you think people who exercise regularly take OTC NSAIDs? Should this change?
What may be an alternative to taking NSAIDs for muscle soreness?
Do you still think it is safe to take NSAIDs for other types of pain, such as menstrual cramps, headaches or fevers?
Further Reading:
Last year’s blog post discussing at delayed recovery after exercise due to NSAIDs

I’m surprised there hasn’t been more studies/awareness about this topic. I know doctors have prescribed these drugs to me after surgery, but in that case the inflammation is due to a different cause. I’m not sure if that would make a difference in their effectiveness– there could be a study about the different types of inflammation being treated with these OTCs. Although it would probably be hard to quantify the results since pain from menstrual cramps isn’t something you can measure. Outside of the anti-inflammatory drugs maybe ice baths or muscle rollers could help relieve pain due to DOMS. I know for me, anti-inflammatory drugs always seem to make me feel better so I’ll continue using them.
In addition to being a weak/ineffective pain reliever for DOMS, evidence is also mounting to support that NSAIDs, such as ibuprofen, are detrimental to musculoskeletal tissue (muscle, tendon, bone) healing following acute injury. The drugs likely act by impeding the natural inflammatory process that initiates the healing cascade. The research has been slowly making its way to inform clinical practice.
If it is true that NSAIDs are detrimental to healing following an acute injury, would there be any use for those type of medicines at all? Are they still effective at helping with aches and pains that may be on a much smaller scale? And how long do you think it may take to come up with an alternative to NSAIDs for pain management?
In regards to the 2006 study, everyone has different pain tolerances. So that may impede the results. In regards to NSAIDS, I don’t like how people are using them to get back into exercising faster. If your body is inflamed, your body is telling you it needs time to heal. So don’t turn off your body’s natural protection to exhaust your muscles more. If you use NSAIDS just to recuperate, that’s fine in my opinion since you’ll be relaxing as your body wanted you to.
I have gone through phases where I get DOMS after my lifts, but I have never used ibuprofen or Advil for it. Personally, I took a longer-term solution to it. If I’ve been out of the gym for a while I slowly increase my way back up which has helped, because in the past when I jumped right back in that was when I experienced the worst DOMS. But what I found helped me the most was fixing my diet to eat healthier foods. When I did this, I was able to workout harder and was less sore than ever. I do take NSAIDs for things like cramps and headaches and will continue to since they seem to help me unless good evidence comes out that proves I shouldn’t.
I thought this post was really interesting. I play club ultimate frisbee for UD and tournaments are long with many people often getting injured or experiencing muscle soreness at tournaments. On Saturdays we normally play 4, hour and a half long games and Sundays we play 3 of those games against a variety of other schools at the tournament. With 10 and a half hours of potential playing time almost everyone on the team will take ibuprofen at some point during the tournament. I am very against using pain medications when we are at tournaments because if I’m injured I’d rather hurt in order to know how bad my injury is to determine whether I can play through it or if I really should be sitting out. The fact that these studies show painkillers do more harm than good is a great reason as to why I go about injuries/soreness in this way. Hopefully I can use these research articles to convince my teammates to avoid painkillers too.
I think this was a really interesting topic because I’ve spent my entire life in a various exercise settings and in every one of them they recommended taking Advil to combat any soreness before a big match or event. So I am surprised that this research is not being spread throughout the exercise community because if it does not help and can aggravate exercise induced small intestine injury then why would anyone continue taking them? I know for me personally whenever I would take Advil after a work out it would make mess with my stomach and I had to stop taking it so it would inhibit me working out for the next few days so it is kind of nice to know that this is a widespread effect from the medication and not just me. But it does make me question the effectiveness of taking NSAIDS for things like cramps and headaches because if they gave me a placebo effect with soreness are they just doing the same with the other symptoms? I hope this information can spread quickly to the CrossFit and HIIT community because I know a lot of people that take NSAIDS to get through the next work out of the day and end up injuring themselves or pulling something so it would definitely be good for them to know that Advil actually is not helping them and that they should listen to their bodies.
I always avoid NSAIDs whenever possible since I hate the idea of not getting the benefits from my workout by blocking the inflammation/related protein synthesis. However, since exercise and aging is my particular area of interest, I have seen some evidence to indicate there are benefits for older adults in using NSAIDs to complement resistance training (see example: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3064281/), likely due to decreasing the overall inflammation that occurs with aging to get more out of their workout.
Despite the evidence against NSAIDs for DOMs and how many of my classmates do not take them for sports related pain, I would like to see the results of a study that compares NSAIDs to no treatment as well as a placebo. The study conducted by Donnelly et al would have made a much better study if there was also a group who completed the downhill runs without any treatment. It would also improve the study to have the same people perform with each treatment group so that each person can act as their own control against variations in pain tolerance. A study like this I would find interesting because this would show if taking a pill helps to mentally persuade the athletes that they are feeling better as compared to taking absolutely nothing for the pain.