By: Elspeth Grasso, Dan Owens and Laura Sturgill
Recommended Further Reading:

By: Elspeth Grasso, Dan Owens and Laura Sturgill
Recommended Further Reading:
Most athletes have heard the term, “no pain, no gain” at one point or another in their athletic careers, but this saying is truer than one might think. Having grown up in a household where sports were played year round, it was common to take over the counter non-steroidal anti-inflammatory drugs (OTC NSAIDs), such as ibuprofen or aspirin to ease the pain. Ran too far? Easy solution, take some Advil. Overdo it with the lifting? Take a few Motrin and you’ll be ready in the morning. It was even common to take these over the counter drugs before a workout, as a way to get a head start on the pain.

Ibuprofen, a common OTC NSAID.
Is there any validity to this solution? OTC NSAID’s are known for their ability to reduce fevers and minor aches and pains. With that being said, are they really useful for exercise related injuries or pains? Specifically, are they safe and effective to use for delayed onset muscle soreness (DOMS) due to exercise?
DOMS is the pain and stiffness that is felt typically between 24 and 72 hours after the workout has been completed but can last up to 7 days. After a strenuous workout, the body responds with acute inflammation as a natural way to heal the body. This inflammation usually goes hand in hand with DOMS, but the specifics of this relationship have not been clearly defined. Many athletes try to combat this by taking ibuprofen (or other OTC NSAIDs) to ease the pain, but recent studies have shown that this isn’t necessarily a foolproof plan.
In a 2006 study completed by Nieman et al., the influence of ibuprofen was measured during the 160-km Western States Endurance Run on endotoxemia (the presence of endotoxins in the blood), inflammation and plasma cytokines. The study included 29 ultramarathoners who consumed 600 and 1200mg ibuprofen the day before and on the race day, respectively, and 25 controls that competed in the race but did not take ibuprofen or any other medications. Blood and urine samples were collected the morning prior to and immediately following the race, and subjects recorded muscle soreness during the week following the race using a 10-point Likert scale. It was found that ibuprofen use compared to non-users did not alter muscle soreness or damage. In addition ibuprofen use was linked to elevated indicators of endotoxemia and inflammation. One limitation of the study was that it did not have a placebo group due to ethical concerns from the race director, but they may have had an impact on the results. In addition, race conditions are not the best conditions to conduct an experiment under, as they can cause extra stress on the body, affecting the results.
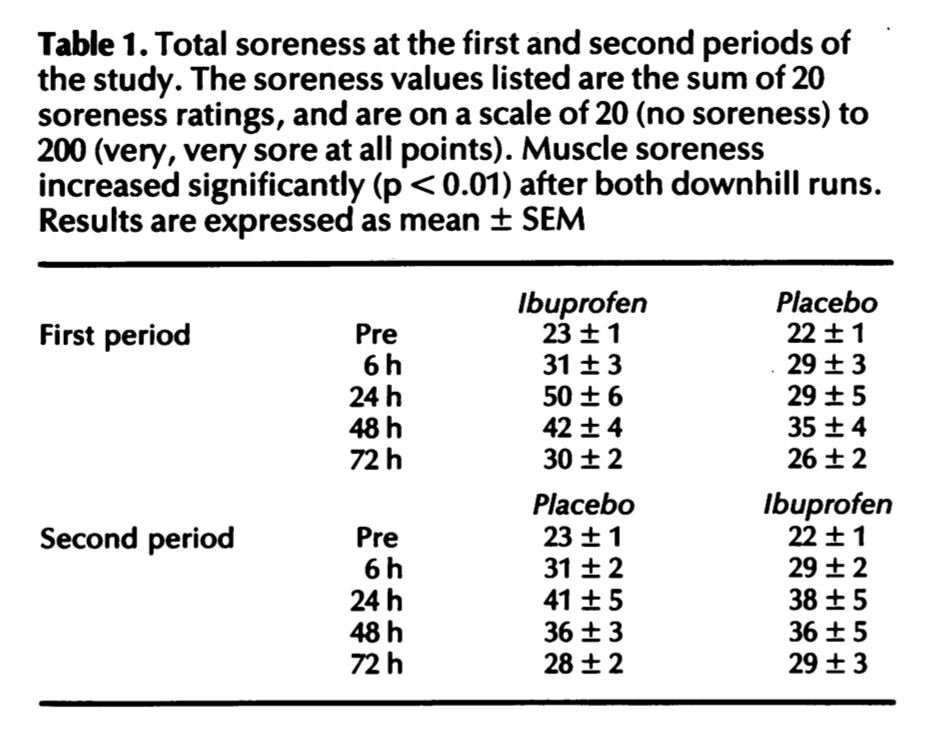
In another study conducted by Donnelly et al., 32 volunteers participated in a study in which ibuprofen was tested against an identical placebo for its effectiveness in reducing muscle soreness and damage after two periods of downhill running. Volunteers took two 600mg ibuprofen or placebo tablets 30 minutes before each run, and took one 600mg tablet every six hours up to 72 hours post-exercise. Blood samples were drawn pre- and post-exercise, and at 6, 24, 48 and 72 hours and analyzed for indicators of muscle damage and inflammation. A questionnaire was used to determine muscle soreness for different regions of the body (the results can be seen in Table 1). The results indicated that ibuprofen is not an appropriate treatment for DOMS and muscle damage. However, one limitation of this study was that during the 10 week break between the two periods of running, there was no monitoring or control of the participants, which means their lifestyles could have been very different from each other, thereby affecting the results.
Furthermore, it is known that exhaustive physical activity leads to small intestinal injury and short-term loss of gut barrier function in otherwise healthy individuals. Another study, conducted in 2012 reveals that ibuprofen aggravates this exercise-induced small intestinal injury and induces gut barrier dysfunction in healthy individuals.
Based on this research, I have concluded that OTC NSAIDs should be discouraged as a way to mitigate the pain that comes with delayed onset muscle soreness. The data from the first two studies show that ibuprofen (and implied other NSAIDs) are not a satisfactory way to decrease the pain that comes from delayed onset muscle soreness. The third study shows that ibuprofen can be extremely harmful to the user and therefore should not be taken if it can be avoided. Based on this information, not only should OTC NSAIDs not be taken for DOMS, but the relationship between inflammation and DOMS should be more thoroughly investigated. It could be that the inflammation isn’t causing DOMS and that is why the drugs aren’t relieving the pain. However, the first study suggests that the intake of ibuprofen increased inflammation, the exact opposite of what it was supposed to do. Either way, ibuprofen and other NSAIDs should not be taken for relief from DOMS.
Questions to consider:
Do you take OTC NSAIDs such as ibuprofen or Advil when you are feeling sore after a hard workout? Do they help? Will you continue?
How often do you think people who exercise regularly take OTC NSAIDs? Should this change?
What may be an alternative to taking NSAIDs for muscle soreness?
Do you still think it is safe to take NSAIDs for other types of pain, such as menstrual cramps, headaches or fevers?
Further Reading:
Last year’s blog post discussing at delayed recovery after exercise due to NSAIDs
The media often puts their own spin on the news in order to make a statement or point of some sort. After reading Chapter 5 of David Epstein’s The Sports Gene, it is apparent that this can be traced back all the way to the 1928 Olympic Games in Amsterdam (Epstein, 59-60). After the women’s 800m run in 1928, John Tunis of the New York Evening Post reported, “Below us on the cinder path were 11 wretched women, 5 of whom dropped out before the finish, while 5 collapsed after reaching the tape.” This reporting caused the International Olympic Committee to keep the 800m off the program until 1960. It was interesting that a simple news article was able to create this kind of power and able to change the Olympic Games.
I researched more about this specific race and came across this article (here), which reported the actual facts of that race. Roger Robinson, a senior writer for The Running Times, describes the race in detail, noting that there were actually only 9 runners in the race, as opposed to the 11 originally reported. Only one of them fell, and not from exhaustion, but instead because she was leaning forward to try to lean forward to beat her competitor. A photo of the winner was captured, Germany’s Lina (Karoline) Radke-Batschauer, in which she shows no signs of exhaustion. According to Robinson, not only was this race false reported in the New York Evening Post, but in other newspapers as well. For example, newspapers said that women’s reproductive capability impaired by such “terrible exhaustion.” England’s Daily Mail affirmed that women who raced longer than 200m would age prematurely.
The fact that these reports were able to convince the IOC that the women’s 800m should no longer be a part of the Olympic Games shows what kind of influence the media has on our culture. It banned the 800m for over 30 years, simply because these reporters thought that women couldn’t handle such a race. Even in 1967, when the first woman ran in the Boston Marathon, she received a lot of criticism and disbelief, with people saying that there was slim to no chance that she would be able to win (read more about her experience here). It is shocking that people’s opinions can influence the rules of sporting event so drastically. Today, with social media, this problem is even more prevalent than before. Opinions are publicized from many different parties, not only confusing people, but sometimes distributing incorrect information. When discussing the issue of nature versus nurture when it comes to athleticism, it is important to consider how the media has influenced opinions in the past and present, as it can cause some serious misconceptions.
Works Cited:
Epstein, David J. The Sports Gene: Inside the Science of Extraordinary Athletic Performance. 2014.
Robinson, Roger. “‘Eleven Wretched Women.’” Runner’s World, 16 May 2017, www.runnersworld.com/running-times-info/eleven-wretched-women.
Switzer, Kathrine. “Boston, 1967: When Marathons Were Just for Men.” BBC News, 16 Apr. 2012, www.bbc.com/news/magazine-17632029.
In a review published in Sports Health, Neeru Jayanthi discusses the evidence for and against sports specialization in young athletes, specifically those under the age of 12. He begins by defining sport specialization as intense, year-round training in a single sport with the exclusion of other sports. He then compiles a table that succinctly displays the results of his literature review. He has reviewed 12 studies, in which he has identified the type of sport, type of athletes involved in the study, age at which they began their training of the sport, and the age at which they specialized. With the exception of two studies, both of which studied rhythmic gymnastics, the studies showed that most elite athletes had diversified early and specialized after 12 years of age. He goes on to discuss other factors that may impact success in sports, such as personal enjoyment of the sport and self-motivation. Lastly, he discusses how injury and burnout may be a result of high-intensity training. He concludes by stating that some specialization is needed to attain elite-level skills, however, it should be delayed until late adolescence to minimize injury and burnout.
This is a similar conclusion that was drawn by David Epstein in The Sports Gene. He too seems to conclude that early specialization may be harmful instead of beneficial to children aiming for elite status in a sport. He agrees that some sports do require early specialization, such as gymnastics, but that is only because they are able to perform at this elite level before they go through puberty. Otherwise, based on the studies he has reviewed, it doesn’t seem required to attain this level (Epstein, 51-52).
I agree with the conclusions drawn from both Jayanthi’s review, as well as Epstein’s. Early diversification allows for children to gain experience in multiple sports, allowing them to acquire skills that may be beneficial. Just like it is encouraged for students to study many different subjects in order to work both sides of their brains, and to be well-rounded students, the same can be said for athletes. Not only does diversification prevent burnout and injuries, but perhaps it could possibly aid the athlete in seeing the sport in a new way, eventually taking what he or she has learned from previous sports and applying it to their specialized sport. Even certain professional athletes today didn’t specialize until much later, if ever. For example, Danny Ainge, who is currently the general manager for the Boston Celtics, is the only player to be named a high school first team All-American in football, basketball and baseball. He then went on to play basketball at Brigham Young University, where he also played professional baseball for three seasons with the Toronto Blue Jays. After, he went on to play for the Celtics. There are other players like him, who were double or even triple sport college athletes. Did not specializing hurt their careers? Or did it help them? Could they have been even better at one sport if they had specialized? I like that this article also took into account (briefly) motivation and enjoyment of the sport. That isn’t something that has been discussed in the book yet, and I am excited to see what Epstein has to say about it.
Read the article here.
Works cited:
Epstein, David J. The Sports Gene: Inside the Science of Extraordinary Athletic Performance. 2014.
Jayanthi, Neeru, et al. “Sports Specialization in Young Athletes: Evidence-Based Recommendations.” Sports Health, 5(3), Apr. 2013, 251–257.