Many people envision an evening under the hands of a masseuse as the perfect example of a relaxing experience, even as those hands dig deep into the “hurts so good” territory. This is often justified with the long term effects promised as the gain to the pain, such as relief of chronic pain, reduced soreness, and feeling looser. These claims are primarily backed by anecdotal evidence rooted in experiences of clients ranging from casual massage goers to professional athletes, as well as from those of practitioners.
Ubiquitously coined by masseuses, physical therapists, and athletic trainers, myofascial release is one of those deep soft tissue massage techniques that gets people excited to let them above their personal pain thresholds. But does myofascial release have any scientific evidence behind it’s effectiveness?
But what really is myofascial release?
The theory is that a primary factor in muscle tightness and pain is the condition of the sticky, gooey web that holds our muscle fibers together and to other parts of our body.

Fig 1: Fascia around and between layers of muscle
Originally posed by physician Stephen Typaldos came the idea that virtually all musculoskeletal injuries were due to distortions of connective tissue, particularly when sticky masses of fascia clump in between muscular fibers. Myofascial release is the practice of, in theory, releasing these fascial clumps to relieve tension on the musculoskeletal system. Dr. Typaldos found a lot of success in his career by using rubbing, friction, sliding, and pulling on acute pain- success that has inspired practitioners to adopt his strategies and aim for the best results. However, while clumps of fascia melting away is easy to visualize, there is no scientific proof that distortions actually exists, nor that they can be removed by manual work. Some argue that fascia doesn’t even matter while others swear by it and pose theories to back their claims, but currently the mechanism, if any, behind myofascial release is unknown.
There is also no common consensus over how myofascial release is really used. For example, some professionals apply myofascial release to trigger points, which don’t seem to be related to fascia at all as per the video below:
Of course, for anyone looking for relief from pain and soreness myofascial release sounds like a good idea, but the costs of repetitively visiting therapists and masseuses is a deterrent. Thus enters the market of self myofascial release including products such as rollers and massage tools, where one can supposedly achieve myofascial release at home without the need of a practitioner. However, things get a little murky here as well – some argue that these techniques can’t actually achieve myofascial release, and there is no proof in either direction:
https://www.youtube.com/watch?v=BnYdzaoMyQ8
Ultimately, these grievances are rooted in the lack of understanding over the mechanism behind myofascial release. Even as these techniques aren’t tightly defined, we’re still left wondering the question: “But does it work?”
Does the massage work?
This one is tricky to answer, using scientific evidence, as there is a lack of high quality, highly controlled studies I myofascial release massage. A 2013 review on the effect of myofascial release on adults with orthopedic conditions found only 10 peer reviewed articles on the topic. Of these, 6 were case studies of which 5 had degrees of improvement ranging from slight to full recovery, and one on which the treatment failed. Of course, there is no way of knowing if massage really had any effect on those results. Of the studies, it was found that in treating plantar fasciitis, hamstring tightness, and misaligned pelvis myofascial release was useful (especially in plantar fasciitis, with on average 60% better pain reduction than the group without three months down the line!. However, the study with the largest subject was on low back pain, in which it was found that myofascial release did improve back pain, but no better than other manipulation techniques. There was no control in this study, however, so again it’s hard to tell if time alone healed all the subjects. With only one randomized control study (plantar fasciitis), I concurred with the authors here that there was a greater need for stronger studies on the subject.
A 2017 review looked only at randomized controlled trials where individuals and personnel were blinded to which treatment group they belonged in. Only 8 were found, all of which indicated myofascial release was beneficial. The conditions studied were tennis elbow and low back pain. Among these, two of them found that myofascial release on top of physical therapy was more useful than just physical therapy.
As we can see here, there really aren’t many conclusive studies on the matter, without a big enough sample of studies to draw a consensus from. I’ll agree it looks like from what we’ve seen myofascial release therapy seems to help, but only two of the above studies actually compare it to fake massage or other massage techniques. While those two studies found myofascial release was better than faking a massage, two are hardly enough to conclude that myofascial release is responsible for reduced pain and not just any massage. Looking at a third study, we see that there is no significant difference between myofascial release and Swedish massage in pain symptoms.
Okay…but what about foam rollers?

An example of a foam roller
Many people use foam rollers as a cheaper alternative to hands on massage to achieve myofascial release. It doesn’t look like we’re sure if myofascial release is even a real thing, but let’s not just go throwing our rollers out feeling dejected and lied to all along. Even if we aren’t sure how foam rollers work, they may still help.
One study looked at 20 gym-going males and how foam rolling affected them while doing a resistance squat and jump height protocol. They were evenly and randomly split into a foam rolling group and non foam rolling group. The study found that throughout their training which consistent of five consecutive days of exercise, the group that foam rolled had consistently lowered muscle soreness and improved range of motion at each time point. The participants that foam rolled did not have better gains in their squat one rep max, but did have better jump height improvement in comparison to the control. One limitation of this study is that the control group had no replacement to foam rolling, such as just laying down on foam, after their workouts, so there could have been another factor involved in the difference between the two groups.
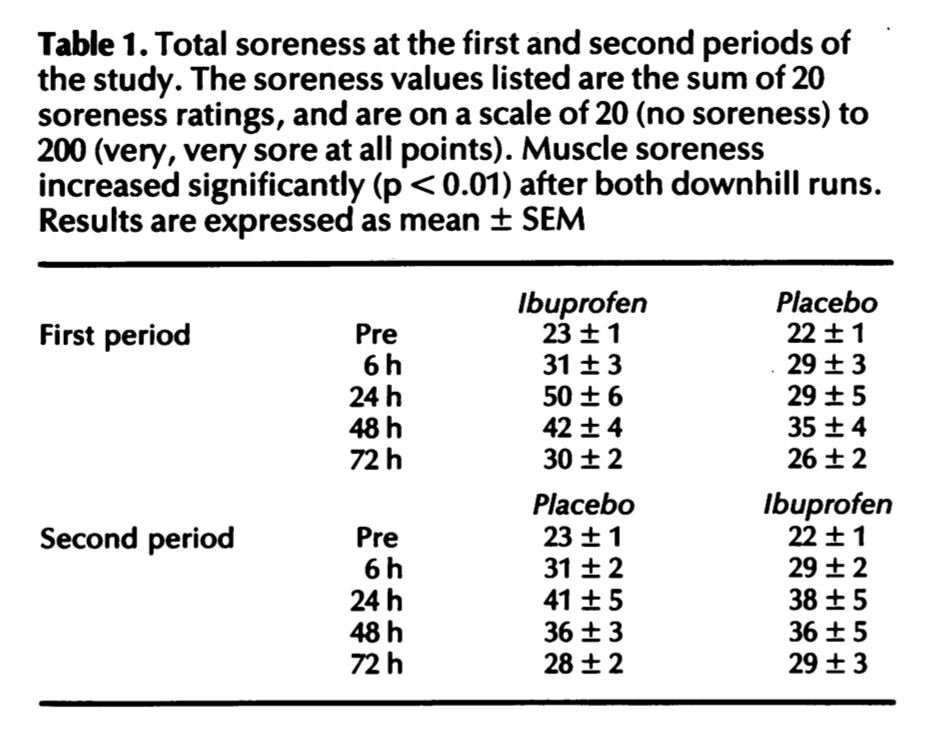
Another study looked at the effect of foam rolling in delayed onset muscle soreness (DOMS), in which a squat regiment was used to induce the pain in both the no foam rolling and foam rolling group, who foam rolled immediately afterward the workout and then 24 hours later and 48 hours later for 20 minutes each time. The foam roller group had significantly reduced muscle soreness and increased tenderness of the quadriceps. The athletes had recorded performance measures such as sprint time and squat reps before the DOMS protocol, and the group the foam rolled had less reduction of performance 24, 48, and 72 hours after. Again, we can say the lack of a more robust control condition applies here, but again the results are promising.
So lets roll it all together
Even though it looks like overall we’re really not too sure what myofascial release massage is, how it works, or if its effective, we can still draw some conclusions from the research. The first is that myofascial release isn’t harmful. With neither the foam rollers or the manual massage did pain increase for subjects or performance decrease. Its true that myofascial release could be no different than any other massage in it’s effects, but they trend to show that whether or not a release of clumps of fascia occurs, the massage does help with pain for certain cases. The same thing goes for foam rolling the legs. Maybe no form of release is occurring at all, but spending the time to foam roll is showing to increase flexibility and reduce soreness at least over the span of time that DOMS is a factor. Importantly, there is no case here to say that if you feel like myofascial release helps you that there is any reason to give it up.
Questions to Consider:
Is it important to know how myofascial release works or just that it does work? If you had limited resources and to support one of those two types of studies, which would it be?
Are randomized controlled trials important to understanding how effective myofascial release is? Or is that being too strict, and looking at case studies and less controlled studies is sufficient enough? Why?
References:
Meltzer, K. R., Cao, T. V., Schad, J. F., King, H., Stoll, S. T., & Standley, P. R. (2010). In vitro modeling of repetitive motion injury and myofascial release. Journal of Bodywork and Movement Therapies, 14(2), 162–171. doi: 10.1016/j.jbmt.2010.01.002
Whitehead, M., Jeffrey, E., khurana, A., Gail, Oster, D., Wilson, S., … Miller, C. (2018, March 8). Self Myofascial Release- What is MFR and how does it work? Retrieved from https://deeprecovery.com/is-myofascial-release-real/
Ingraham, P. (n.d.). Fascia Science Review. Retrieved from https://www.painscience.com/articles/does-fascia-matter.php#sec_origins
Problems MFR Helps. (n.d.). Retrieved from https://www.myofascialrelease.com/about/problems-mfr-helps.aspx
American Fascial Distortion Model Association. (n.d.). Retrieved from https://afdma.com/
Mckenney, K., Elder, A. S., Elder, C., & Hutchins, A. (2013). Myofascial Release as a Treatment for Orthopaedic Conditions: A Systematic Review. Journal of Athletic Training, 48(4), 522–527. doi: 10.4085/1062-6050-48.3.17
Laimi, K., Mäkilä, A., Bärlund, E., Katajapuu, N., Oksanen, A., Seikkula, V., … Saltychev, M. (2017). Effectiveness of myofascial release in treatment of chronic musculoskeletal pain: a systematic review. Clinical Rehabilitation, 32(4), 440–450. doi: 10.1177/0269215517732820
Liptan, G., Mist, S., Wright, C., Arzt, A., & Jones, K. D. (2013). A pilot study of myofascial release therapy compared to Swedish massage in Fibromyalgia. Journal of Bodywork and Movement Therapies, 17(3), 365–370. doi: 10.1016/j.jbmt.2012.11.010
Macdonald, G. Z., Button, D. C., Drinkwater, E. J., & Behm, D. G. (2014). Foam Rolling as a Recovery Tool after an Intense Bout of Physical Activity. Medicine & Science in Sports & Exercise, 46(1), 131–142. doi: 10.1249/mss.0b013e3182a123db
Pearcey, G. E. P., Bradbury-Squires, D. J., Kawamoto, J.-E., Drinkwater, E. J., Behm, D. G., & Button, D. C. (2015). Foam Rolling for Delayed-Onset Muscle Soreness and Recovery of Dynamic Performance Measures. Journal of Athletic Training, 50(1), 5–13. doi: 10.4085/1062-6050-50.1.01