Anyone who has partaken in any physical activity, whether it is a sport, exercise routine, or just simple around the house chores that require a little more muscle power than normal, has experienced muscle soreness or discomfort. Generally, when muscles are pushed passed what they are used to (i.e. new exercising routines, increased weight, eccentric exercises) the muscle fibers undergo damage and the body’s response is to add muscle fibers and/or to increase the size of muscle fibers to help increase muscle strength. When talking about sore muscles, it is generally thought the soreness comes from the physical effects of muscle tearing, repairing, and growing from a workout. There is, however, one part of the muscle that plays a role in not only soreness, but also range of motion (flexibility), and muscle performance that not many people know needs special attention: the myofascial tissue.
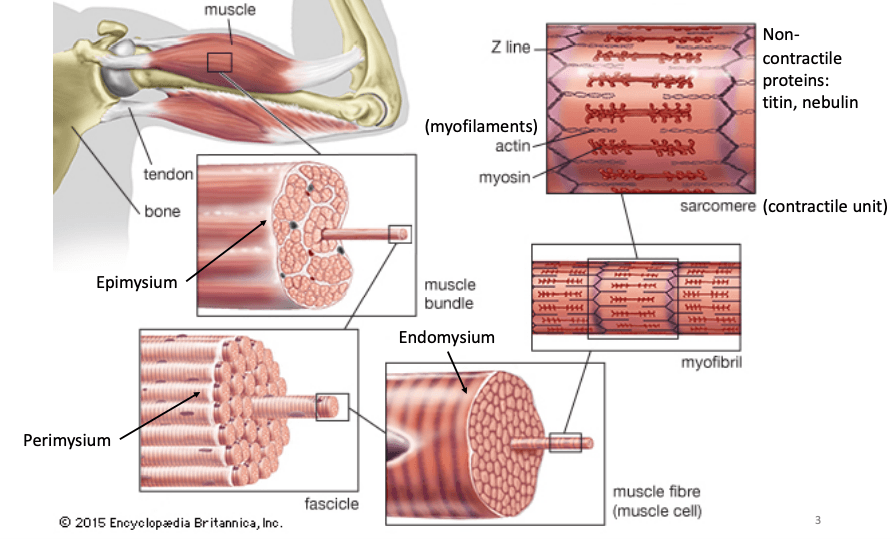
Figure 1: Skeletal muscle structure through different layers of the muscle. Myofascial tissue lies over the epimysium connective tissue which coats the muscle bundle. The epimysium, perimysium, and endomysium are specialized versions of myofascial tissue.
Different forms of fascia can be found all over the body, from encasing organs, to blood vessels and nerves, to muscle. Fascial tissue that specifically covers muscle, or myofascial tissue, is a thin, white/transparent connective tissue that covers muscle, bundles, muscle fibers, and the muscle as a whole. If you have ever picked off the thin white stuff covering parts of a chicken breast while preparing it for dinner, you tore off the myofascial tissue layer. Myofascial tissue is an extremely flexible and strong material, which is made up of elastin fibers, for stretch, and collagen fibers, for strength, that are embedded in a gelatinous ground substance, which reduces friction between the muscle fibers and promotes ease of motion [1]. Considered a “deep fascia,” myofascial tissue is made up of a more compacted weave than other fascia found throughout the body and can modify itself depending on the forces placed on it. (Figure 2). Because of this, if there is “trauma” or “injury” to the tissue, it can become out of alignment and

Figure 2: 3D visualization of myofascial tissue (white web like structure) and fascia tissue between the skin and muscle (yellow web like structure). Myofascial tissue can be related to a cotton candy structure that is extremely complex and strong. Retrieved from https://www.myofascialrelease.com/about/definition.aspx
cause trigger or dysfunctional points. These points, most commonly referred to as knots, is when the fibers that make up the tissue gets stuck together, loses its elasticity, and becomes taught [2]. Polly de Mille, R.N., C.S.C.S., director of performance services at the Hospital for Special Surgery in New York City explains in an interview for SELF that it is very similar to getting ice cream in silky smooth hair. When there are “knots” in the muscle fascia, it limits range of motion, and can trigger immune responses which can ultimately lead to pain and discomfort (cytokines have been shown to cause pain and soreness) [3,4].
Now, what is the best way to heal and prevent muscles from experiencing these knots and discomfort? When talking about getting rid of knots in your body, a massage should be the first thing that comes to mind. The “hurts so good” mentality of deep massaging muscles to where the patient feels pain and then relief afterwards is a popular desire, though not for everyone. Applying pressure and different forces to the tissue through a massage, or foam roller which we will talk about in a little bit, while moving around the fascia helps to separate and relax the tissue and muscle, allowing it to go back to its natural state. Effects also include an increase in blood flow, which should help muscles get the proper nutrients to repair. Massaging also releases “feel good” brain chemicals, like endorphins, which basically inhibit pain receptors and overall makes you feel better. A study conducted by Mal-Soon Shin and Yun-Hee Sung induced muscle fatigue on 21 young males and treated 11 of them to massages afterwards while recording surface muscle activation and position of their medial gastrocnemius muscle. According to their study, massaging increases muscle activation and strength due to a change of structural properties. However, in their discussion, they mention that not all messages are effective, which seems to be a common issue in the argument of whether foam rollers, or self myofascial release in general, works or not [5].
Massages are so great because when another person is working out your muscles, they are not only more accurate in pinpointing the location, but they can also apply more force (remember: collagen is EXTREMELY strong in ratio to its size. Proportionally, it is stronger than steel!). As great as they are, unless someone at home is a masseuse, it can be costly. Self myofascial release techniques, such as foam rolling, have taken over the exercise world and are now regularly used. Foam rolling is when the user applies pressure to “trigger point” or sore spot before or after a workout by using their body weight to roll against a foam cylinder. Though it feels good, does it actually work?
Research has proven that foam rolling is great for warming up muscles and increasing range of motion and flexibility, but the verdict is still out on decreasing muscle soreness. Though the mechanism behind foam rolling is not exactly known, there is great evidence that it does work on some type of level, whether it is physical or just simply mental. In a systematic literature review of research on using a foam roller before and after workouts, Scott W. Cheatham identified different scientific articles that were critically appraised with trusted conclusions. From these articles, he identified five studies on the effects of foam rolling and range of motion before exercising. All of these studies resulted with an increase in stretching or range in motion in test subjects [6]. It is common knowledge to stretch before a workout or game to help “warm up” the muscles so that they’re are more flexible, which helps prevent injury and soreness. It is also speculated that rolling out could create a friction that literally heats up the fascia and muscle, making it more flexible and the typical “loose” feeling [2]. After a workout, however, there is a preconception that rolling out will help with delayed onset muscle soreness and pain in general. In this literature review, Cheatham identifies two different journals that conclude that foam rolling does reduce pain, but since the mechanism behind it is still unknown, how much can we trust? In the same SELF article as mentioned previously, Lewis J. Macgregor, Ph.D., an exercise physiologist and lead author of the University of Stirling confirms foam rolling does help increase blood flow, which in turn promotes muscle recovery, but foam rolling does not actually help with myofascial release. Since the collagen in the fascia is so strong, it is argued using your body weight to roll out is not enough. Instead, the pressure of rolling stimulates nerve receptors, which sends the same “hurts so good” feeling to your brain that is then perceived as loosening up the muscle, when really it is not happening.
Overall, foam rolling and myofascial release is an effective way to warm up your muscles and stretch them out before a workout and to help stimulate more blood flow post workout, just don’t get your hopes up about avoiding soreness! Increasing range of motion and flexibility before a workout is a great step to ease muscle soreness, but foam rolling alone is not the answer. The verdict is still out on the mechanism behind the effects of myofascial release on a cellular level, but hey, if it feels good, why not!
If you’re interested, here is a video of foam rolling techniques because like anything, it’s not effective if you don’t do it properly.
https://www.youtube.com/watch?v=WCj1dvTwOF0
Questions to consider:
Is it worth it to foam roll or stretch in general before physical activity?
Is myofascial release something to think about daily and not just dealing with exercising?
Do you think foam rolling has a placebo effect or is it both systems (nervous and skeletomuscular) working together?
Do you think foam rolling is just another exercising fad?
Would adding heat be beneficial? Or a waste of time?
Sources:
- Shah, S., & Bhalara, A. (2012). Myofascial Release. International Journal of Health Sciences and Research,2(2), 69-77.
- Fetters, K. A. (2018, July 21). Here’s What Foam Rolling Is Actually Doing When It Hurts So Good. Retrieved April 12, 2019, from https://www.self.com/story/what-foam-rolling-is-actually-doing-when-it-hurts-so-good
- Grosman-Rimon, L., Parkinson, W., Upadhye, S., Clarke, H., Katz, J., Flannery, J., … Kumbhare, D. (2016). Circulating biomarkers in acute myofascial pain: A case-control study. Medicine, 95(37), e4650. doi:10.1097/MD.0000000000004650
- Zhang, J. M., & An, J. (2007). Cytokines, inflammation, and pain. International anesthesiology clinics, 45(2), 27–37. doi:10.1097/AIA.0b013e318034194e
- Shin, M., & Sung, Y. (2015). Effects of Massage on Muscular Strength and Proprioception After Exercise-Induced Muscle Damage. Journal of Strength and Conditioning Research,29(8), 2255-2260. doi:10.1519/jsc.0000000000000688
- Cheatham, S. W., Kolber, M. J., Cain, M., & Lee, M. (2015). THE EFFECTS OF SELF-MYOFASCIAL RELEASE USING A FOAM ROLL OR ROLLER MASSAGER ON JOINT RANGE OF MOTION, MUSCLE RECOVERY, AND PERFORMANCE: A SYSTEMATIC REVIEW. International journal of sports physical therapy, 10(6), 827–838.