
Identify
Heart rate monitors are useful for athletes, researchers, and clinicians as a method of assessing fitness and cardiovascular health. Heart rate is a basic measure that clinicians use to monitor patients and typically do so with electrocardiogram (ECG). ECG is not as easy to measure upon movement and often requires larger, non-portable measurement devices. For athletes who seek to measure heart rate during exercise, these heart rate monitors are found in the form of a watch or chest strap. Despite its wide-use and high level of reporting, user activity can affect heart rate monitor accuracy. For LED heart rate monitors, where a light is emitted onto the user’s skin as opposed to electrodes that rest on the surface of the skin in ECG, position of the device on the body (Figure 1) and user activity can potentially affect the heart rate data. The issue of erroneous data is especially prevalent for multisport athletes who engage in activities that require different body positions and movements.

Obtaining consistent heart rate data collection and analysis is essential for being able to compare data across activities. For example, an athlete may have a reported average heart rate over a cycling activity as 110bpm and 140bpm during a running activity. Is this difference is due to different intensities for each activity or is it due to inconsistencies in data collection due to different noise factors dependent on activity?
Being able to identify characteristic noise frequencies based on user activity and monitor placement can greatly benefit athletes. This will allow users to either change the placement of the device based on their activity or, more favorably, input the activity to the device prior to data collection, allowing the device to prepare different filtering techniques based on expected noise for that particular activity. Applying these filters to the device would enhance heart rate monitor design and better ensure accurate data.
Formulate
Before solving this problem, a basic understanding of heart rate monitors is necessary. LED heart rate monitors emit a green light to the user’s skin. Some of this light is absorbed, and some is reflected back into a receiver within the device. The absorption can be modeled using the Beer-Lambert law, A = ε𝓁c, where absorbance (A) is equal to absorptivity (ε), beam length (𝓁), and concentration of absorbing species (c) [4].
The intensity of the light, based on absorbance, is evaluated by a photodiode in the receiver and is transformed into a photoplethysmogram (PPG) signal by the device’s processor. This PPG signal contains cardiac, respiratory, and motion data, as well as noise. Filters act to remove non-cardiac components from the PPG signal [1] – this is where heart rate data error can occur if not enough noise is removed (Figure 2). Since motion is a noise component in the PPG signal, heart rate data can be influenced by monitor position and user activity [2].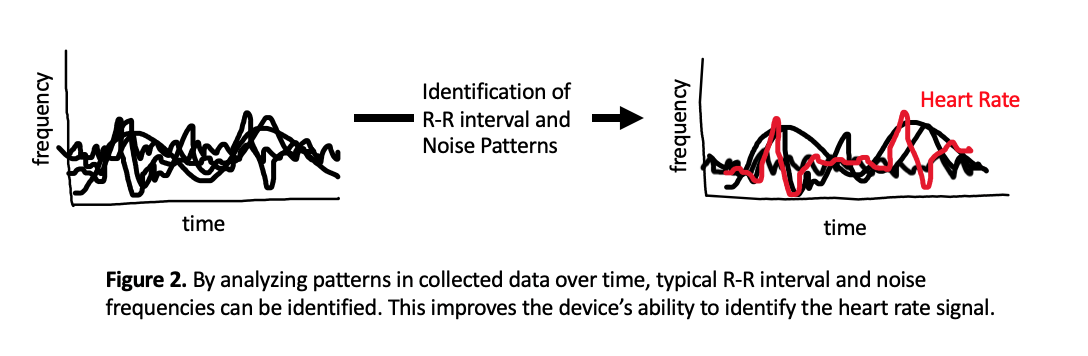
To assess potential discrepancies in heart rate data based on monitor position and user activity, two heart rate monitors can be worn in different locations during various activities (Figure 1). In data collection, it is important to know heart rate data for each of these monitor placements over time at rest and during different activities. It is also important to use a ECG monitor as a reference (i.e a verified, widely-used chest strap) to know what heart rate data should be.
Assumptions made in solving this issue is that light intensity emitted from the heart rate monitor device is consistent throughout an activity, all activities, and between devices. Another assumption is that user intensity for each activity is the same such that heart rate increases are due to monitoring differences rather than increased workout intensity. PPG signal will also be assumed to only have components of cardiac (i.e. heart rate) signals and non-cardiac noise signals. These assumptions allow for heart rate output due to device position and activity to be determined.
Solve
Solving the problem of heart rate monitor outputs varying based on user activity and device position first requires an understanding of which device placements respond to different activities. This data is collected from users wearing monitors in different positions and engaging in different activities. It has been determined that wrist-based measurements respond better to walking and running activities than forearm measurements while forearm measurements respond better to cycling activities than wrist measurements (Figure 3). Both respond well to rest [2].

Next, an analysis of the PPG signal generated for each device placement and each activity can be completed. This allows for the determination of frequencies that are characteristic of noise in each of these activities. For example, since cycling creates more noise in wrist measurements than forearm measurements, the PPG signals of each of these measurements can be compared to determine what is present in the wrist signal that is not present in the forearm signal. This discrepancy, say frequency A, is noise generated in wrist measurements due to cycling motion.
Performing this analysis on a large data set of heart rate measurements over different device placements and user activities allows for the identification of noise frequencies characteristic of certain user activities. In designing a heart rate monitor device, these frequencies can be programmed to be filtered out based on the activity being completed. For example, a user can select “cycling” on their wrist based heart rate monitor prior to beginning exercise and the device will then apply the filter to remove frequency A noise from the data, producing heart rate data just as accurate as a forearm monitor. Designing devices such that noise can be correctly identified and removed will allow multisport athletes to gain reliable heart rate data regardless of activity and without having to move their device on their arm.
This solution is reasonable, however determining exact frequencies characteristic of certain activities would require large data sampling since there is much individual variation in heart rate. Limitations stem from assumptions mentioned above, as user intensity is often not constant across activities and emitted light intensity may change throughout an activity as the device moves closer and farther from the user’s skin due to motion.
References
[1] P. R. MacDonald and C. J. Kulach, “Heart Rate Monitoring with Time Varying Linear Filtering,” US 9801587 B2, 2017.
[2] J. Parak and I. Korhonen, “Evaluation of wearable consumer heart rate monitors based on photopletysmography,” 2014 36th Annu. Int. Conf. IEEE Eng. Med. Biol. Soc. EMBC 2014, pp. 3670–3673, 2014, doi: 10.1109/EMBC.2014.6944419.
[3] J. L. Cheng, J. R. Jeng, and Z. W. Chiang, “Heart rate measurement in the presence of noises,” 2006 Pervasive Heal. Conf. Work. PervasiveHealth, 2006, doi: 10.1109/PCTHEALTH.2006.361651.
[4] D. F. Swinehart, “The Beer-Lambert law,” J. Chem. Educ., vol. 39, no. 7, pp. 333–335, 1962, doi: 10.1021/ed039p333.

